Have We Pharmaceuticalised Sadness?

There is a very specific kind of discomfort that comes from realising how quickly women’s distress can be turned into a diagnosis, a prescription, or a neat little label.
You are exhausted, anxious, flat, overwhelmed, crying before your period, numb after having a baby, irritable in perimenopause, burnt out from trying to be thin, productive, emotionally available and successful at the same time. And instead of asking what your body and life might be trying to tell you, the conversation often jumps straight to brain chemistry.
I want to be clear from the beginning. This is not about shaming anyone who takes antidepressants. Medication can be life-saving. In severe depression, suicidal crisis, OCD, panic disorder, debilitating anxiety, postnatal depression, PMDD, or when someone simply cannot function, SSRIs can be part of a proper care plan. Nobody should ever stop an antidepressant suddenly or without medical support.
But I also think we need to be much more honest about how casually antidepressants have become the answer to very complicated human problems. Because for many women, the first serious conversation should not be, “Which SSRI shall we try?” It should be, “What is actually happening in your body, your hormones, your sleep, your relationships, your nutrition, your trauma history, your nervous system and your life?”
Not every woman who is struggling has a Prozac deficiency. Sometimes she is sleep deprived. Sometimes she is under-eating. Sometimes she is lonely. Sometimes she is inflamed, depleted, grieving, hormonally shifting, unsupported, overworked, vitamin D deficient, in a relationship that is slowly draining her, or living in a body that has been ignored for far too long.
And if we reduce all of that to “your serotonin is low”, we miss the point.
How We Got Here
The history of antidepressants is actually quite recent. Modern antidepressants began in the 1950s, when drugs such as iproniazid and imipramine were found to improve mood, partly by affecting neurotransmitters like serotonin, noradrenaline and dopamine [1]. These discoveries helped shape the monoamine theory of depression, which suggested that depression might be linked to low levels of certain brain chemicals.
Then came SSRIs, or selective serotonin reuptake inhibitors. The most famous one, fluoxetine, better known as Prozac, was approved by the FDA in 1987 and became culturally huge in the late 1980s and 1990s [2]. SSRIs work by blocking the reuptake of serotonin, which means more serotonin remains available in the synaptic space between nerve cells [3]. In simple terms, they change serotonin signalling.
That is not the same thing as proving depression is caused by a simple serotonin deficiency.
This distinction matters because the “chemical imbalance” explanation became one of the most powerful mental health narratives of the last few decades. It was simple. It was reassuring. It made depression feel biological rather than moral. For many people, that was genuinely helpful, because it reduced shame.
But the science has always been more complicated.
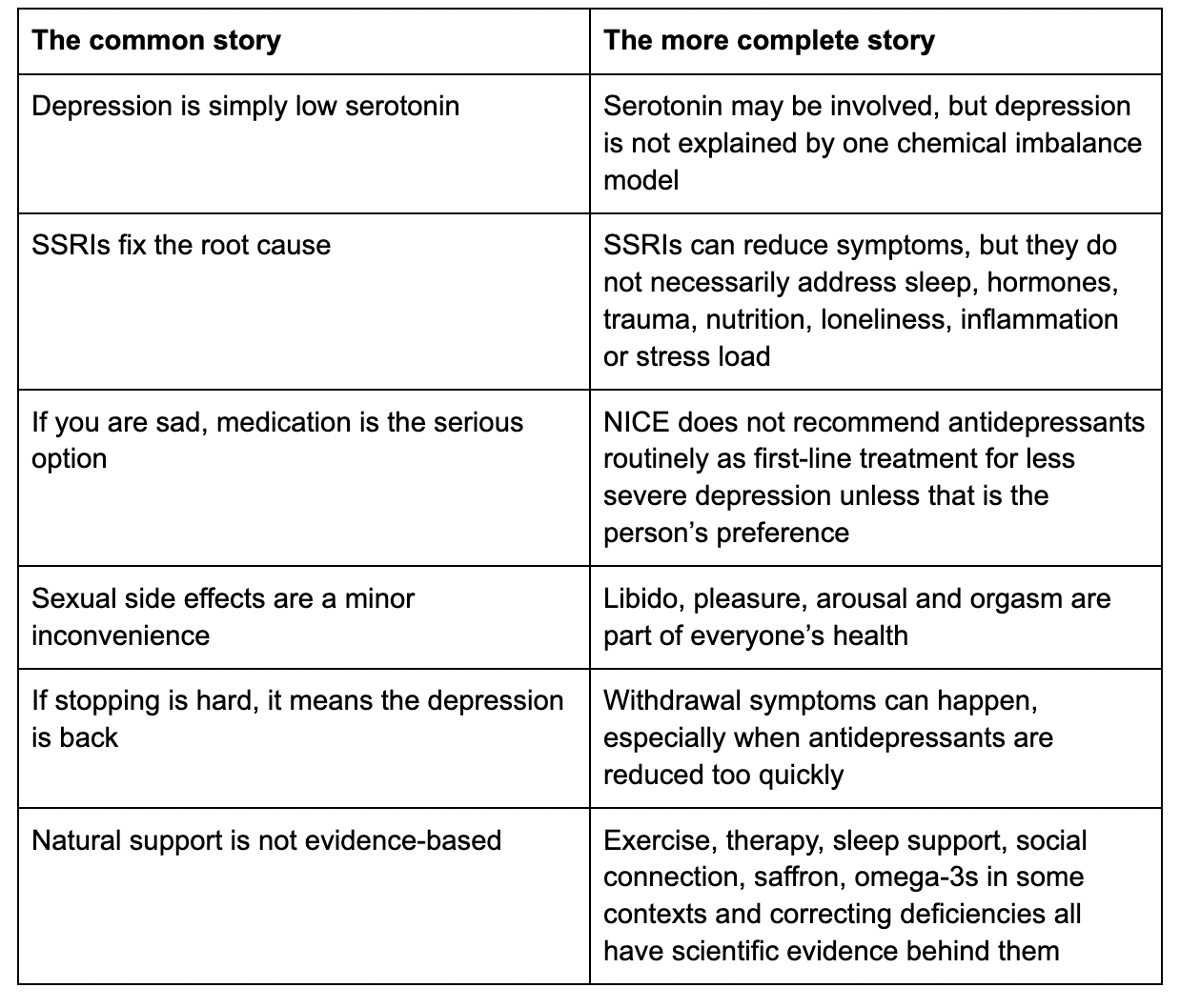
A major 2022 umbrella review in Molecular Psychiatry concluded that the main areas of serotonin research do not provide consistent evidence that depression is caused by lowered serotonin activity or concentrations [4]. That does not mean SSRIs never help. It means the story we were sold was too neat.
And women have often been the target audience for neat stories.
The Problem Is the One-Size-Fits-All Story
SSRIs are among the most commonly prescribed medications in the UK. NHS data has shown a substantial rise in antidepressant prescribing in England over the past decade, with tens of millions of antidepressant items dispensed each year [5]. Some of this may reflect reduced stigma and more people seeking help, which is a good thing.
But it should also make us pause.
Why are so many people, and especially so many women, struggling? Why are we so quick to individualise distress? Why is the first serious intervention so often medication, when so many root causes are lifestyle, relational, hormonal, nutritional, inflammatory, environmental or social?
Even NICE guidance in England does not recommend routinely offering antidepressants as a first-line treatment for less severe depression, unless that is the person’s preference [6]. That is important. Because the public conversation often makes it sound like antidepressants are the obvious next step for anyone who feels persistently low. They are not.
In many cases, first-line care should mean proper assessment, therapy, sleep support, nutritional support, movement, social connection, blood tests where appropriate, and an honest look at the person’s actual life. Not because medication is evil. Because depression is not usually one thing.
It is often accumulation.
Poor sleep. Low protein. Low iron. Low vitamin D. Blood sugar crashes. Alcohol. Loneliness. Childhood attachment wounds. Grief. Relationship heartbreak. Trauma. Hormonal shifts. Perimenopause. Postnatal depletion. Burnout. Chronic stress. A job that eats your soul. A life where you are constantly performing wellness but never actually feel safe.
Of course you might feel depressed. It would almost be strange if you felt completely happy while living through something genuinely hard.
This is where I think we need to question our method. We have started to pathologise normal responses to difficult life circumstances. If someone is grieving, lonely, exhausted, undernourished, overworked or traumatised, their sadness is not necessarily a random malfunction. It may be an intelligent signal.
That does not mean we leave people to suffer. It means we stop pretending the only respectable form of help comes in a blister pack.
SSRIs Can Help, But They Are Not Neutral
There is good evidence that antidepressants can be more effective than placebo for adults with major depressive disorder over the short term, although the size of benefit varies between medications and between people [7]. So the question is not, “Do antidepressants ever work?” They can.
The better question is, “Have we made them carry a burden they were never designed to carry?”
Medication cannot make a woman feel safe in a relationship that is draining her. It cannot replace sunlight, protein, iron, sleep, friendship, touch, purpose, community or a menstrual cycle that is being wrecked by under-fuelling and over-exercising. It cannot process trauma for her. It cannot make burnout disappear if the person keeps living in the exact conditions that created it.
And SSRIs are not neutral sweets. They are medications with effects, side effects and trade-offs.
Common side effects can include nausea, sleep changes, digestive symptoms, headaches and changes in appetite or weight [3]. Sexual side effects are also very common, including reduced libido, difficulty becoming aroused and difficulty reaching orgasm [8]. For women, this is not a small side note. Libido, pleasure and sexual function are part of health.
Some people also describe emotional blunting on SSRIs. Not everyone does, and some people feel more like themselves because their anxiety or depression lifts. But for others, life can feel like it has been turned down. Less panic, yes, but also less desire, less creativity, less joy, less sexual aliveness, less emotional range. That matters.
There is also the issue of withdrawal. NICE now explicitly recognises that withdrawal symptoms can be mild for some people, but can also be more severe and last longer for others, particularly if antidepressants are stopped suddenly [6]. Reported symptoms can include dizziness, flu-like feelings, insomnia, irritability, electric shock sensations, anxiety and mood changes [3] [6].
This is why I think the conversation around SSRIs needs to become more honest. Starting them can be easy. Coming off them can be really hard. For some women, what was framed as a short-term support slowly becomes something they feel trapped on for years.
Again, this is not about fear. It is about informed consent.
Women deserve to understand what they are taking, why they are taking it, what the alternatives are, what the exit plan is, and what else might be driving their symptoms. A prescription without a wider conversation is not holistic care. It is symptom management.
Who Benefits When Women Stay Medicated But Unsupported?
I know “Big Pharma” can sound like something people say when they have gone too far down the internet. But we also cannot pretend the pharmaceutical industry has always behaved like a benevolent public health charity.
The history is dark. Purdue Pharma’s marketing of OxyContin is one of the clearest examples of how aggressive pharmaceutical marketing can reshape prescribing and cause devastating harm [9]. The Sackler family and Purdue have been widely scrutinised for their role in promoting OxyContin, and the same wider history includes Arthur Sackler’s earlier marketing work on tranquillisers such as Librium and Valium [10].
SSRIs are not opioids, and we should not collapse every medication into the same story. But the broader lesson matters. Pharmaceutical companies are not neutral educators. They are businesses. They benefit when more people take medication for longer.
So when millions of people are on antidepressants, we are allowed to ask who benefits from a culture where sadness, grief, burnout, loneliness and hormonal upheaval are so often treated as individual brain disorders.
It is not “conspiracy” to ask that. It is health literacy.
Women’s Mental Health Has Always Been Too Conveniently Pathologised
Women’s distress has a long history of being treated as a problem inside women, rather than a response to the world around them.
We have moved from hysteria to tranquilisers to antidepressants to the modern wellness internet where everyone is “dysregulated”, “burnt out”, “oestrogen dominant”, “low dopamine” or “needing to fix their cortisol”. The language has changed, but the pattern can be surprisingly similar. A woman feels something. Culture tries to package it.
This does not mean women’s symptoms are not real. They are very real. PMS, PMDD, postnatal depression, perimenopausal mood changes, anxiety, panic, burnout and depression can be devastating. Hormones absolutely affect mood, cognition, sleep, appetite, libido and emotional regulation.
But women’s emotional symptoms are often treated in isolation from the body they are happening in.
A woman on the pill who feels emotionally flat may be told she is just anxious. A woman in perimenopause may be offered an antidepressant before anyone properly discusses oestrogen, progesterone or HRT. A woman who is under-eating and training six days a week may be treated as disciplined until her period disappears and her mood crashes. A new mother may be expected to cope on broken sleep, no village and one six-week GP check. A woman who is lonely may be told to meditate.
This is where the conversation needs to change.
Mental health is not separate from the body’s physical health. The brain is an organ. It needs blood sugar stability, thyroid hormones, sex hormones, micronutrients, sleep, movement, sunlight, social safety and inflammatory balance. It is not floating above the rest of you having private serotonin problems.
The Natural Supports We Should Be Taking Seriously
When I say natural support, I do not mean “just go for a walk and stop complaining”. I hate that. Depression is not a bad attitude. Anxiety is not a failure of gratitude. Severe mental illness needs proper care.
But I also think the word “natural” has been unfairly made to sound unserious. There are many non-pharmaceutical supports that have real evidence behind them. They are not always enough on their own, but they should be part of the conversation far more often than they are.
And really, these are not “alternative” foundations. They are foundations.
Therapy, Trauma and Actually Being Heard
If depression is connected to trauma, attachment, grief, heartbreak, chronic stress or feeling unsafe, then the answer cannot only be serotonin. Therapy matters because it gives context to symptoms. It helps people understand patterns, process what happened, build emotional regulation, and stop blaming themselves for responses that may once have been protective.
NICE recommends a range of psychological therapies and guided self-help options for depression, especially in less severe cases [6]. That matters because therapy is not a luxury add-on after medication fails. For many people, it should be part of the first serious conversation.
Sometimes the problem is not that your brain is broken. Sometimes your nervous system adapted beautifully to something painful, and now it needs help learning that life is different.
Movement Is Not Just About Looking Good
Exercise is one of the most evidence-backed interventions for depression. A 2024 BMJ systematic review and network meta-analysis of 218 randomised trials involving more than 14,000 participants found that exercise was associated with reductions in depressive symptoms, with walking or jogging, yoga, strength training, mixed aerobic exercise and tai chi or qigong all showing benefit [11].
This does not mean you need to punish yourself with brutal workouts when you are already exhausted. In fact, for many women, over-exercising can be part of the problem. The goal is not to use exercise as another way to control your body. The goal is to move in a way that helps your nervous system remember it is alive.
For some people that is lifting weights. For others it is walking, Pilates, dancing, yoga, swimming or taking a class where you feel part of something. The best exercise is the one you can actually repeat without hating your life.
Saffron Is More Than a Pretty Spice
Saffron is one of the natural compounds I find genuinely interesting for mood. A meta-analysis of randomised clinical trials found that saffron supplementation significantly improved depressive symptoms compared with placebo in adults with major depressive disorder. Trials comparing saffron with antidepressants found no significant difference between groups, although the authors emphasised the need for larger and longer studies [12].
That does not mean saffron is a magic replacement for medication. It means it deserves attention. If you are on antidepressants or other medication, you should always check with a qualified practitioner before adding supplements, because natural does not automatically mean risk-free.
But this is exactly my point. We should be able to talk about saffron seriously without pretending it is witchcraft or a miracle.
Omega-3s, Brain Cell Membranes and Inflammation
Omega-3 fatty acids, especially EPA and DHA, are structural components of neuronal cell membranes and are involved in inflammatory pathways, which makes them relevant to brain health and mood [13]. Research on omega-3s for depression is mixed, but some studies suggest benefit, particularly for EPA-dominant formulas or as an add-on support in some people [13].
This is where personalised health matters. If someone eats oily fish regularly, their needs may be different from someone who does not. If someone is inflamed, undernourished or has very low omega-3 intake, supporting fatty acid status may be more relevant.
Again, it is not about one supplement fixing your life. It is about asking whether the brain has the raw materials it needs.
Vitamin D Is Not a Personality Trait
Low mood in winter is not always mysterious. Vitamin D receptors are found in the brain, and vitamin D is involved in immune and inflammatory regulation. A 2023 systematic review of randomised controlled trials found mixed evidence for vitamin D supplementation in depression, with five of eight studies showing positive effects and three showing no significant benefit [14]. The authors concluded that the evidence is not strong enough to call vitamin D an established depression treatment, but it may be relevant, especially when deficiency is present [14].
This is the kind of nuance we need more of. Vitamin D is not an antidepressant. But if your levels are low, correcting that is basic body care. Sometimes the “root cause” is not deep. Sometimes it is that you have barely seen sunlight, you are deficient, and your body is asking for help.
Sleep Is Not Optional If You Want a Stable Mind
I know sleep advice can sound boring, but sleep is one of the least sexy and most profound mental health interventions we have. A meta-analysis of 34 prospective cohort studies involving more than 172,000 participants found that insomnia was significantly associated with an increased risk of later depression, with a pooled relative risk of 2.27 [15].
That does not mean insomnia causes every case of depression. But it does show how closely sleep and mood are connected.
From a women’s health perspective, this matters even more because poor sleep affects blood sugar, appetite, cortisol, thyroid function, reproductive hormones and emotional resilience. Nobody feels like their best self when they are running on caffeine, adrenaline and five hours of broken sleep. Sleep is not laziness. Sleep is endocrine care. Sleep is nervous system care. Sleep is mental health care.
Food, Blood Sugar and the Brain You Actually Live In
We cannot have an honest conversation about women’s mood without talking about food. Not in a diet culture way. In a “your brain is made of nutrients and runs on energy” way.
Under-eating, skipping breakfast, living on coffee, fearing carbs, not eating enough protein, drinking alcohol to cope and then wondering why anxiety is through the roof the next day is so common. But common does not mean normal. Blood sugar instability can feel like anxiety. Low iron can feel like depression. Not eating enough can flatten libido, disrupt ovulation, raise stress hormones and make the whole body feel unsafe.
This is why “eat properly” is not basic advice. It is sometimes the missing piece. A nervous system cannot feel safe in a body that is being chronically underfed.
Social Connection Is Biology
We need to stop treating community like a cute lifestyle accessory. Social connection is a health factor.
A 2024 review in World Psychiatry described strong evidence linking loneliness and social isolation with poorer mental health, especially depression [16]. The US Surgeon General has also described loneliness and social isolation as major public health concerns, affecting health through biological, psychological and behavioural pathways [17].
This makes complete sense. Humans are not designed to regulate alone forever. We need conversation, laughter, touch, eye contact, belonging and people who make us feel like ourselves again.
And this is where the modern wellness world can become so strange. We will spend hundreds of pounds on supplements while ignoring the fact that we have not had a proper laugh with a friend in weeks. We will track our HRV but not ask whether our lives feel meaningful. We will optimise everything except the things that actually make us human.
Purpose, Service and Doing Something Beyond Yourself
Purpose is not a fluffy concept. It gives the nervous system a reason to orient outward. It reminds you that your life is not just a project to manage.
Observational research has linked volunteering with lower depression and loneliness in older adults, although this kind of study cannot prove cause and effect [18]. Still, it fits with what many of us intuitively know. Doing something useful, kind or connected can shift you out of self-monitoring and into relationship with the world.
This does not need to be dramatic. It can be volunteering, charity work, helping a friend, joining a community project, mentoring someone, cooking for someone who is struggling, or simply becoming more useful in your own corner of the world.
Sometimes healing is not another hour spent analysing yourself. Sometimes it is remembering that you are needed.
What Women Actually Deserve
Women deserve more than two extremes. We do not need the old medical model that says, “You are chemically broken, take this and be quiet.” And we do not need the online wellness model that says, “You can fix everything naturally if you just try hard enough.”
Both can be cruel.
The truth is much more human. Some women need medication. Some women need therapy. Some women need HRT. Some women need better sleep, more food, fewer punishing workouts, blood tests, sunlight, omega-3s, saffron, vitamin D, friendship, time outside, a new job, a safer relationship, boundaries, grief support, trauma work, or a reason to get up in the morning that is not just productivity.
Most women need a combination.
This is why I think the antidepressant conversation needs to become less polite and more intelligent. Not reckless. Not anti-medicine. Intelligent.
We can acknowledge that SSRIs help some people while also questioning why women’s sadness, overwhelm and hormonal vulnerability are so often treated as isolated brain disorders. We can respect medication while still asking why it has become so normal for women to stay on it for years without a broader plan. We can be grateful for modern psychiatry without pretending Big Pharma has always told women the full story.
The goal is not to reject help. The goal is to widen the definition of help.
If you are struggling, please do not stop medication suddenly, and please do not let anyone online shame you for needing support. But also, please do not let anyone reduce your emotional life to a single neurotransmitter. You are not just a brain in a jar. You are a body, a cycle, a nervous system, a history, a social being, a person with needs.
Maybe there is nothing “chemically wrong” with you in the simplistic way you were told. Maybe life has been hard. Maybe your body has been trying to survive. Maybe your sadness is not proof that you are broken, but a signal that something needs care, change, support, nourishment, honesty or time.
And sometimes the most radical thing we can do is stop asking, “What is wrong with me?” and start asking, “What is my body trying to tell me, what is my life asking me to change, and what kind of support do I actually need?”
Words by Eva Fleischman for The Well Edit.
References
[1] Hillhouse, T. M. & Porter, J. H. (2015). A brief history of the development of antidepressant drugs: From monoamines to glutamate. Experimental and Clinical Psychopharmacology. URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC4428540/
[2] Greenslit, N. & Kaptchuk, T. J. (2012). Antidepressants and advertising: Psychopharmaceuticals in crisis. Yale Journal of Biology and Medicine. URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC3313530/
[3] NHS. Selective serotonin reuptake inhibitors (SSRIs). URL: https://www.nhs.uk/mental-health/talking-therapies-medicine-treatments/medicines-and-psychiatry/ssri-antidepressants/overview/
[4] Moncrieff, J. et al. (2022). The serotonin theory of depression: a systematic umbrella review of the evidence. Molecular Psychiatry. URL: https://www.nature.com/articles/s41380-022-01661-0
[5] NHS Business Services Authority. Medicines Used in Mental Health, England, 2015/16 to 2020/21. URL: https://www.nhsbsa.nhs.uk/statistical-collections/medicines-used-mental-health-england/medicines-used-mental-health-england-201516-202021
[6] NICE. (2022, updated). Depression in adults: treatment and management. Recommendations. URL: https://www.nice.org.uk/guidance/ng222/chapter/Recommendations
[7] Cipriani, A. et al. (2018). Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder. The Lancet. URL: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(17)32802-7/fulltext
[8] NHS. Side effects of SSRIs. URL: https://www.nhs.uk/mental-health/talking-therapies-medicine-treatments/medicines-and-psychiatry/ssri-antidepressants/side-effects/
[9] Van Zee, A. (2009). The promotion and marketing of OxyContin: Commercial triumph, public health tragedy. American Journal of Public Health. URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC2622774/
[10] Keefe, P. R. (2017). The Family That Built an Empire of Pain. The New Yorker. URL: https://www.newyorker.com/magazine/2017/10/30/the-family-that-built-an-empire-of-pain
[11] Noetel, M. et al. (2024). Effect of exercise for depression: systematic review and network meta-analysis of randomised controlled trials. BMJ. URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC10870815/
[12] Hausenblas, H. A. et al. (2013). Saffron (Crocus sativus L.) and major depressive disorder: a meta-analysis of randomized clinical trials. Journal of Integrative Medicine. URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC4643654/
[13] Mehdi, S. et al. (2023). The effects of omega-3 fatty acids on depression and inflammatory markers in patients with depression. Journal of Personalized Medicine. URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC9962071/
[14] Guzek, D. et al. (2023). Effect of vitamin D supplementation on depression in adults: a systematic review of randomized controlled trials. Nutrients. URL: https://www.mdpi.com/2072-6643/15/4/951
[15] Li, L. et al. (2016). Insomnia and the risk of depression: a meta-analysis of prospective cohort studies. BMC Psychiatry. URL: https://link.springer.com/article/10.1186/s12888-016-1075-3
[16] Holt-Lunstad, J. (2024). Social connection as a critical factor for mental and physical health: evidence, trends, challenges, and future implications. World Psychiatry. URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC11403199/
[17] Office of the U.S. Surgeon General. (2023). Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community. URL: https://www.hhs.gov/sites/default/files/surgeon-general-social-connection-advisory.pdf
[18] Mayers, A. et al. (2024). Volunteering, loneliness and depression in older adults. Healthcare. URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC11545050/
Note: This article is for informational and educational purposes only. It is not intended to replace professional medical advice, diagnosis or treatment. If you are taking antidepressants or experiencing severe depression, suicidal thoughts, panic, postnatal depression, PMDD, or significant mood changes, please speak to a qualified healthcare professional. Do not stop or alter prescribed medication without medical guidance.
The content published by The Well Edit is for informational and educational purposes only. It is not intended as, and should not be relied upon as, a substitute for professional medical, health, nutritional, legal, or financial advice. While articles may reference insights from qualified practitioners or experts, the views expressed are their own and do not necessarily reflect the views of The Well Edit. Always seek the guidance of a qualified professional before making changes to your diet, lifestyle, supplementation, or healthcare routine.
Use of any information provided is at your own discretion and risk.